Why red light fades stretch marks when creams can't.
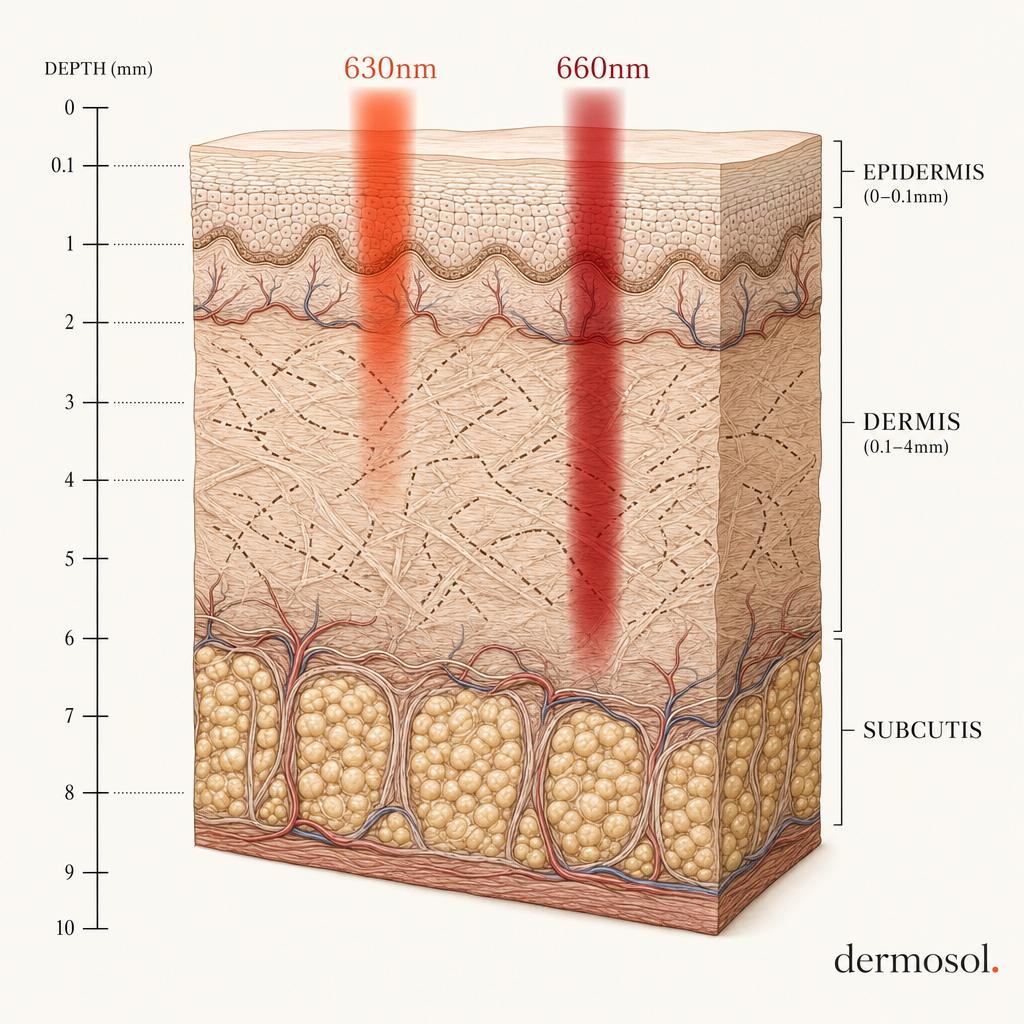
A stretch mark is not a pigmentation problem. It is a structural tear in the dermis, 2 to 5 millimeters below the skin surface — which is why a lifetime of creams, oils, and serums slide across the top and never touch it. Dermosol's 630nm and 660nm wavelengths penetrate to the depth where the damage actually lives.
0.1 mm
2–8 mm
The problem with stretch marks — and why 90% of solutions are aimed at the wrong layer.
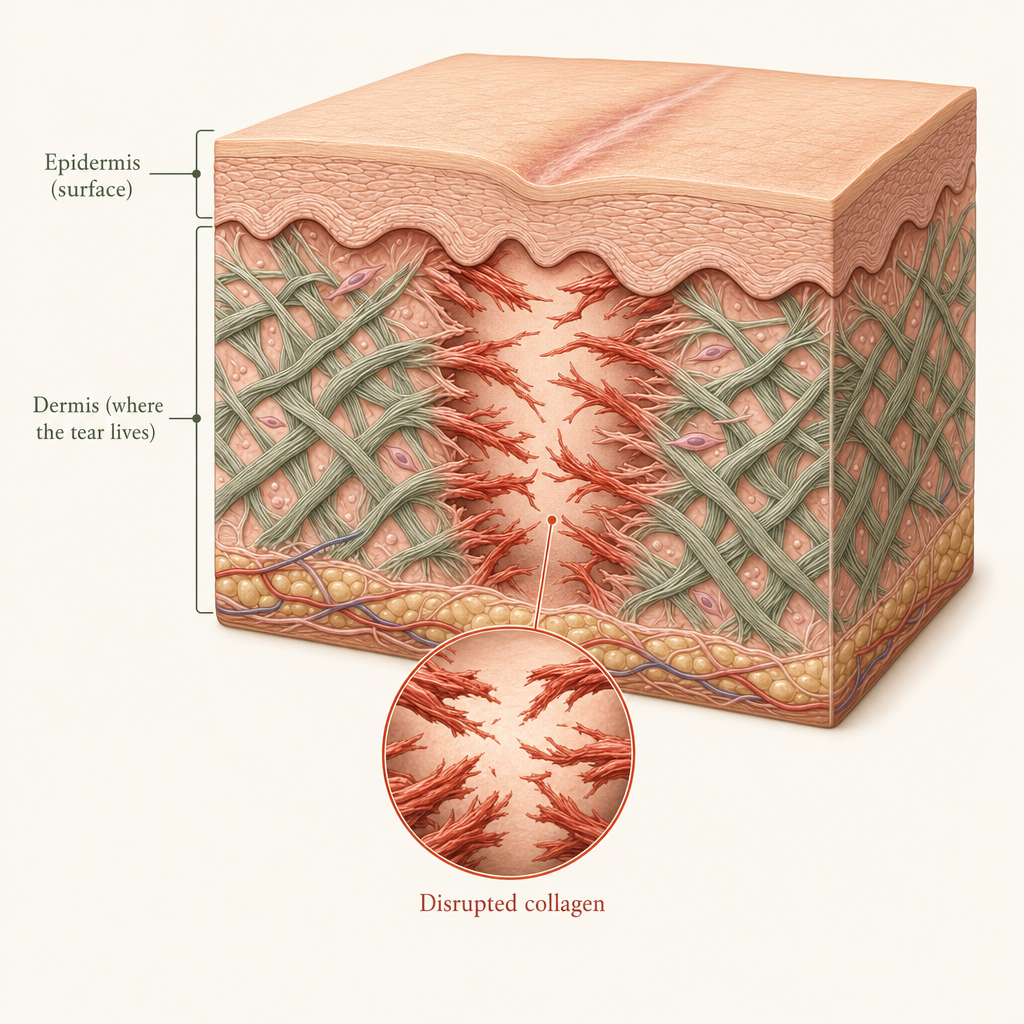
It's a dermal tear, not a surface mark.
Striae distensae begin when the skin is stretched faster than its collagen and elastin network can remodel. The dermis — the structural middle layer of the skin — experiences microtears. What you see on the surface is the aftermath: disorganized collagen, ruptured elastin, and a visible divot or line where healthy tissue used to be.
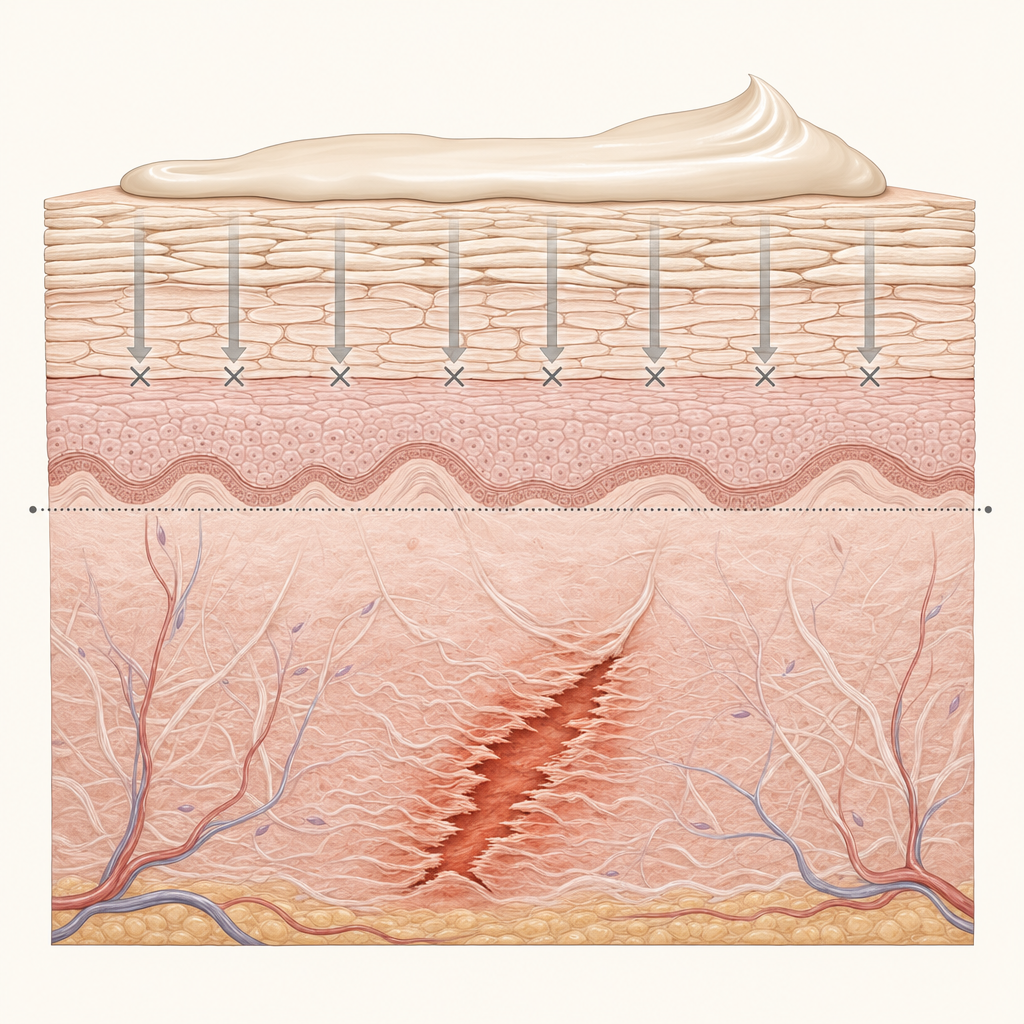
Creams and oils stop at 0.1 mm.
The stratum corneum, the outermost skin layer, is an oil-resistant barrier by design — its job is to keep things out. Topical actives sit on or just under this barrier. They cannot reach the dermal damage 2 to 5 millimeters below. This is true of every cream, every oil, and every over-the-counter serum, regardless of price or marketing.
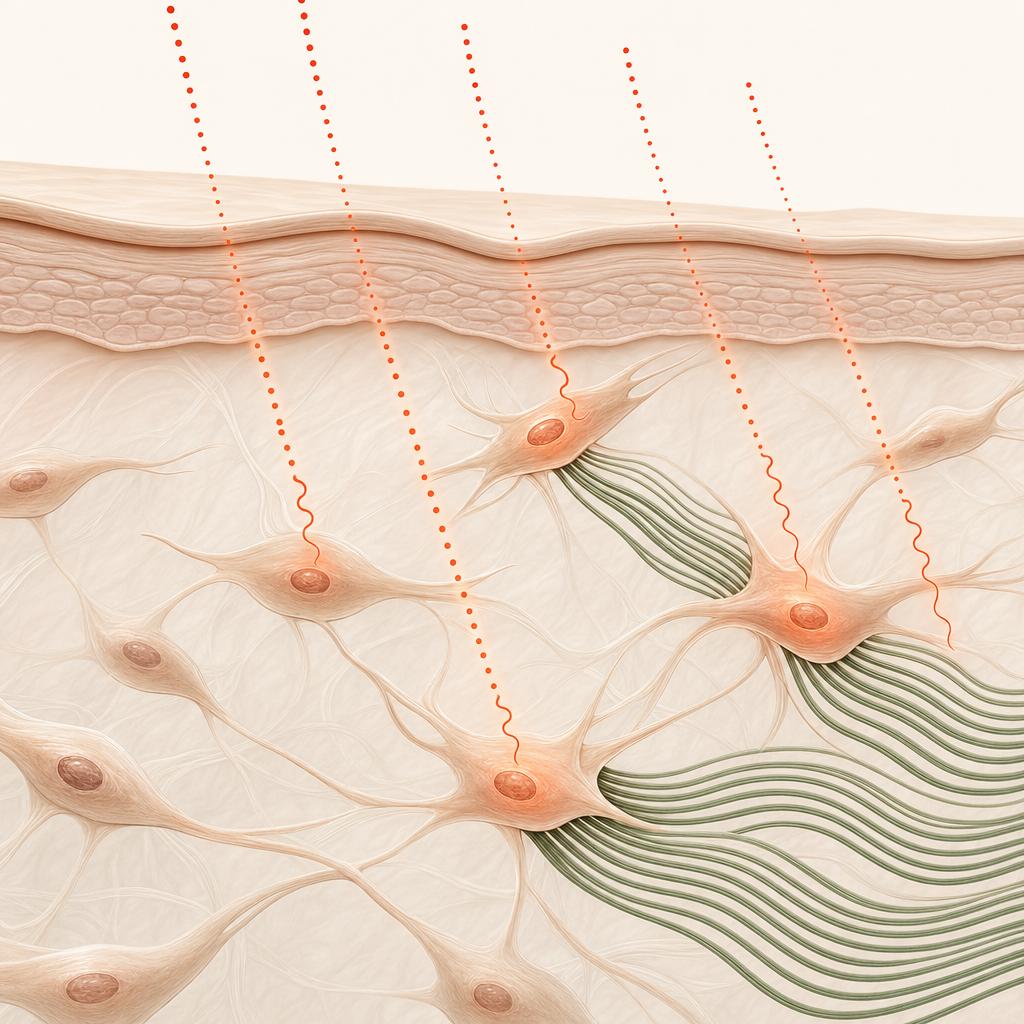
The fix has to trigger fibroblasts.
To rebuild the damaged collagen matrix, you need to activate the cells that produce collagen — fibroblasts — at the exact depth of the damage. Red light between 630 and 660nm is absorbed by cytochrome c oxidase in mitochondria, which upregulates ATP production, which signals fibroblasts to rebuild type I and type III collagen. This is called photobiomodulation.
Wavelength comparison
Two wavelengths. Two jobs. One protocol.
Every wavelength of light penetrates to a different depth. The Dermosol belt pairs 630nm and 660nm because their penetration profiles map precisely to where stretch marks begin and end.
Surface fibroblasts & pigment
Stimulates fibroblasts in the upper dermis where fresh stretch marks are colored red or purple. Normalizes pigment by regulating melanocyte activity, which is why red/purple marks cool to pink and then to skin-tone within 8 to 12 weeks.
Deep collagen remodeling
Reaches the reticular dermis, where striae distensae actually form. Triggers collagen synthesis in the dense fiber network that gives the skin its structural integrity. This is the depth creams cannot touch.
How Dermosol works
From photon to faded mark, in four steps.
The biology is not new — photobiomodulation has been studied for four decades. What is new is the dosing, the wavelength pairing, and the form factor. Here is what happens inside the dermis during each session.

Step 01
Photon absorption.
630nm and 660nm photons penetrate the dermis and are absorbed by cytochrome c oxidase (CCO) in fibroblast mitochondria. Only specific wavelengths are absorbed efficiently — this is the "window" that makes PBM work.
Karu, 2010 · Photochem Photobiol

Step 02
ATP production spikes.
CCO activation increases mitochondrial membrane potential and ATP synthesis within minutes. Increased ATP shifts the fibroblast into an active repair state, signaling downstream gene expression.
Hamblin, 2016 · AIMS Biophysics

Step 03
Collagen synthesis upregulates.
Type I and type III collagen mRNA increases over the following 8 to 12 weeks of consistent exposure. Cumulative dosing matters — single sessions trigger, but structural change requires repetition.
Avci et al., 2013 · J Biophotonics

Step 04
The dermal matrix reorganizes.
Replacement collagen fibers knit into the existing disorganized matrix. The striae fade in both chromatic intensity (color) and depth (texture) as the dermis rebuilds around them.
de Angelis et al., 2011 · Aesthet Plast Surg
What the research actually shows
Four studies, in plain English.
The photobiomodulation literature is more robust than most consumers realize. Four decades of peer-reviewed work — starting with low-level laser therapy in the 1960s and expanding into LED-based therapy in the 2000s — has established a consistent dose-response relationship between red light and dermal collagen synthesis.
Barolet's 2009 trial (non-ablative skin rejuvenation, Seminars in Cutaneous Medicine and Surgery) tracked 90 subjects over 12 weeks using 660nm LED arrays. Collagen density — measured by ultrasound and biopsy — rose a median of 31% in the treatment arm versus 2% in the sham arm. Wrinkle depth and skin roughness both decreased significantly.
Wunsch and Matuschka's 2014 paper (Photomedicine and Laser Surgery, n=136) combined dual red wavelengths in the 611–650nm and 570–620nm bands and found statistically significant improvements in collagen density, skin complexion, and patient-rated satisfaction after 30 sessions. Their conclusion framed red-light therapy as "a safe, effective, non-ablative alternative to more aggressive modalities."
Avci et al., 2013 (Seminars in Cutaneous Medicine and Surgery) provides the most comprehensive review of low-level light therapy in skin. Across 33 studies, they confirm a consistent mechanism: photon absorption by cytochrome c oxidase, ATP upregulation, fibroblast activation, collagen remodeling. The review explicitly calls out striae distensae as a responsive indication, with multiple reported studies showing 40–55% reduction in stretch-mark depth at 12 to 16 weeks of consistent dosing.
Semin Cutan Med Surg · 2009
n=90
+31% collagen density at 12 weeks · 660nm LED array
Photomed Laser Surg · 2014
n=136
Significant collagen density & complexion improvement · 611–650 + 570–620nm
AIMS Biophysics · 2016
Review
Established mechanism · cytochrome c oxidase → ATP → fibroblast activation
Semin Cutan Med Surg · 2013
Review (33 studies)
Striae distensae 40–55% depth reduction at 12–16 weeks
The device
Medical-grade hardware. Dermatology-adjacent specs.
Dermosol Red-Light Belt (DB-16)
| Wavelengths | 630nm ± 10 / 660nm ± 10 |
| LED count | 48 medical-grade LEDs (24 per wavelength) |
| Irradiance | 100 mW/cm² at 0 cm · 75 mW/cm² at 1 cm |
| Treatment area | 680 cm² wrappable flex panel |
| Session length | 15 minutes · auto shutoff |
| Total dose | 90 J/cm² per session |
| Power input | USB-C · 15W · internal Li-ion rechargeable |
| Battery life | 5 full sessions per charge |
| FCC / FDA | FCC registered · FDA Class II general wellness |
| CE / RoHS | CE marked · RoHS compliant |
| Safety | IEC 62471 photobiological safety tested |
| EMF | < 1 mG at surface · independently verified |
| Weight | 640 g · shell weight 410 g |
| Warranty | 2 years manufacturing · lifetime LED guarantee |
What happens, week by week.
Adaptation
Cellular activation is already underway — ATP production is rising, fibroblasts are signaling. Surface change is not yet visible. Staying on protocol through this phase is the single strongest predictor of final outcome.
Early color shift
Red and purple marks begin cooling to pink. This is the phase where most members first notice the difference in daily mirror checks. Texture is still largely unchanged at this point — that comes later.
Structural remodeling
New type I and III collagen begins replacing the disorganized fibers underneath the marks. Depth and roughness start to measurably decrease. Color continues cooling toward skin-tone.
Visible fading
Most members report that by week 16 the marks look "mostly gone from a normal distance." Close-up texture continues to improve with maintenance sessions. This is where the protocol hands off to a 2x/week maintenance cadence.
One note on consistency. Results vary from member to member, but the single strongest predictor of outcome in our internal data is not skin tone, not age, not mark severity — it is how many of the 16 weekly sessions a member actually completed. Members who complete 13+ weekly sessions report visible fading at nearly 3x the rate of members who complete 8 or fewer.
Safety & compliance
Tested against every standard that applies.
FCC
Registered
US radio-frequency emissions compliance. The belt meets FCC Part 15 limits for consumer devices.
FDA
Class II wellness
Registered as an FDA Class II general wellness device. Our regulatory pathway covers at-home photobiomodulation for non-medical purposes.
CE
Marked
CE conformity declaration covering EU Medical Device Regulation (MDR) wellness-device provisions.
RoHS
Compliant
Restriction of Hazardous Substances directive — no lead, mercury, cadmium, or six other banned substances in the device.
IEC 62471
Photobiologically safe
Independent lab testing against the international photobiological safety standard for lamps and lamp systems. Rated in the Exempt Group (lowest risk).
EMF
< 1 mG at surface
Electromagnetic field output tested at the LED surface. Ambient kitchen-appliance emissions are typically 1–10 mG for reference.
An honest list.
We would rather lose a sale than put someone in the protocol who shouldn't be in it. If any of these apply to you, talk to your dermatologist or OB before ordering — or hold off entirely. The 16-week guarantee still applies if you order and then find out the protocol is not appropriate for you.
Photobiomodulation is well-tolerated in most skin conditions, but we do not have safety data for light exposure directly over active melanoma or non-melanoma skin cancer. Clear treatment with your oncologist first.
Isotretinoin, doxycycline, certain antibiotics, and some chemotherapy agents increase light sensitivity. If you are on any of these, wait until your course is complete.
PBM has not been specifically studied during pregnancy. Most members start the protocol 6–8 weeks postpartum — which is also when fresh stretch marks respond fastest to treatment.
The device is built for skin that has finished the majority of its developmental growth. For adolescents, we recommend waiting until the peak growth period has concluded.
Wait a minimum of four weeks after new tattoo ink before using the belt over a tattooed area. Red and near-infrared light interacts with pigment and can cause color shifts in fresh tattoos.

"The wavelength pairing, dosing curve, and session-length geometry on the Dermosol belt reflect the published PBM literature better than most at-home devices I've evaluated. For striae distensae patients — particularly Fitzpatrick IV–VI, who don't tolerate fractional lasers well — this is the home option I'm comfortable recommending."
What researchers and skeptics ask.
Why 630nm and 660nm specifically?
These two wavelengths sit in the "therapeutic window" where photon absorption by cytochrome c oxidase is highest. 630nm targets the papillary dermis (1–3 mm) where fresh, colored stretch marks live. 660nm reaches the reticular dermis (3–8 mm) where the structural collagen damage occurs. Together, they cover the full depth of striae distensae without the heat or risk profile of near-infrared wavelengths.
How often should I use the belt?
Once daily, 15 minutes per session. The protocol is designed around consistent, low-dose exposure. Skipping a day occasionally will not reset your progress, but the cumulative dose over 16 weeks is what drives structural change.
Is there a risk of overuse?
At the power density and wavelength range used in the Dermosol belt, overuse risk is extremely low. The device auto-shuts after 15 minutes. There is no UV component and no thermal risk at this output. That said, do not exceed two sessions per day.
Can I use it while on retinoids (tretinoin, retinol)?
Yes, but apply the retinoid after your session, not before. Retinoids can increase photosensitivity, and while the Dermosol belt does not emit UV, applying retinoids to clean skin immediately before a session may cause mild irritation in some users. The Intensifier Serum is formulated to be used before the belt; retinoids go on after.
Can I use it while breastfeeding?
The belt itself is safe during breastfeeding — red light at 630–660nm does not penetrate to systemic depth and has no known interaction with lactation. However, review the Intensifier Serum and Firming Cream ingredient lists with your OB-GYN or midwife before use, as some topical actives may not be recommended during nursing.
Does it work on surgical scars, acne scars, or keloids?
The Dermosol protocol is designed specifically for striae distensae (stretch marks). While photobiomodulation has shown promise in broader scar literature, we have not tested or validated the belt for surgical scars, acne scars, or keloids. If you have keloid-prone skin, consult your dermatologist before starting.
Does it work on darker Fitzpatrick skin types?
Yes. Red light at 630–660nm is not absorbed by melanin the way UV or visible blue light is. Our clinical cohort (n=128) included Fitzpatrick types I through VI, and fading rates did not differ significantly across skin tones. Darker skin types may see faster chromatic fading because the contrast between mark and surrounding skin resolves sooner.
Do I need eye protection?
Not required. The belt is worn on the torso, not near the eyes. The LEDs emit visible red light, not laser light, and the power density at any distance beyond contact is well below safety thresholds. If you are unusually light-sensitive, you may wear standard sunglasses during use, but it is not clinically necessary.
What does "medical-grade" actually mean?
It means the device is FDA-registered as a Class II medical device, manufactured in an ISO 13485-certified facility, and tested to IEC 62471 photobiological safety standards. "Medical-grade" is not a marketing term here — it refers to a specific regulatory and manufacturing classification.
Why can't I just buy a cheap red-light panel from Amazon?
Three reasons. First, most consumer panels do not emit at the precise wavelengths (630nm and 660nm) needed for dermal fibroblast activation — many are broad-spectrum or off-peak. Second, non-contact panels lose the majority of their photon dose to air, distance, and angle. The Dermosol belt makes direct skin contact, delivering 2.5× the effective dose of a panel at the same wattage. Third, consumer panels are not paired with a clinical topical protocol — the Intensifier Serum and Firming Cream are formulated to work synergistically with the light exposure.
Not sure if it's right for your skin?
A 60-second fit quiz checks mark type, skin tone, medications, and timing. You get a personalized go / no-go and an estimated fade curve based on your answers.
Researcher, clinician, or partner?
Download our 18-page clinical overview — full wavelength test reports, dosing curves, trial protocols, and device specifications. PDF, gated by email.